National Scleroderma Awareness Month – June 2025

- Posted by Greg Wahlstrom, MBA, HCM
- Posted in Health Observance Calendar
Hospital Leadership in Rare Autoimmune Disease Strategy and Equity
Published: June 1, 2025
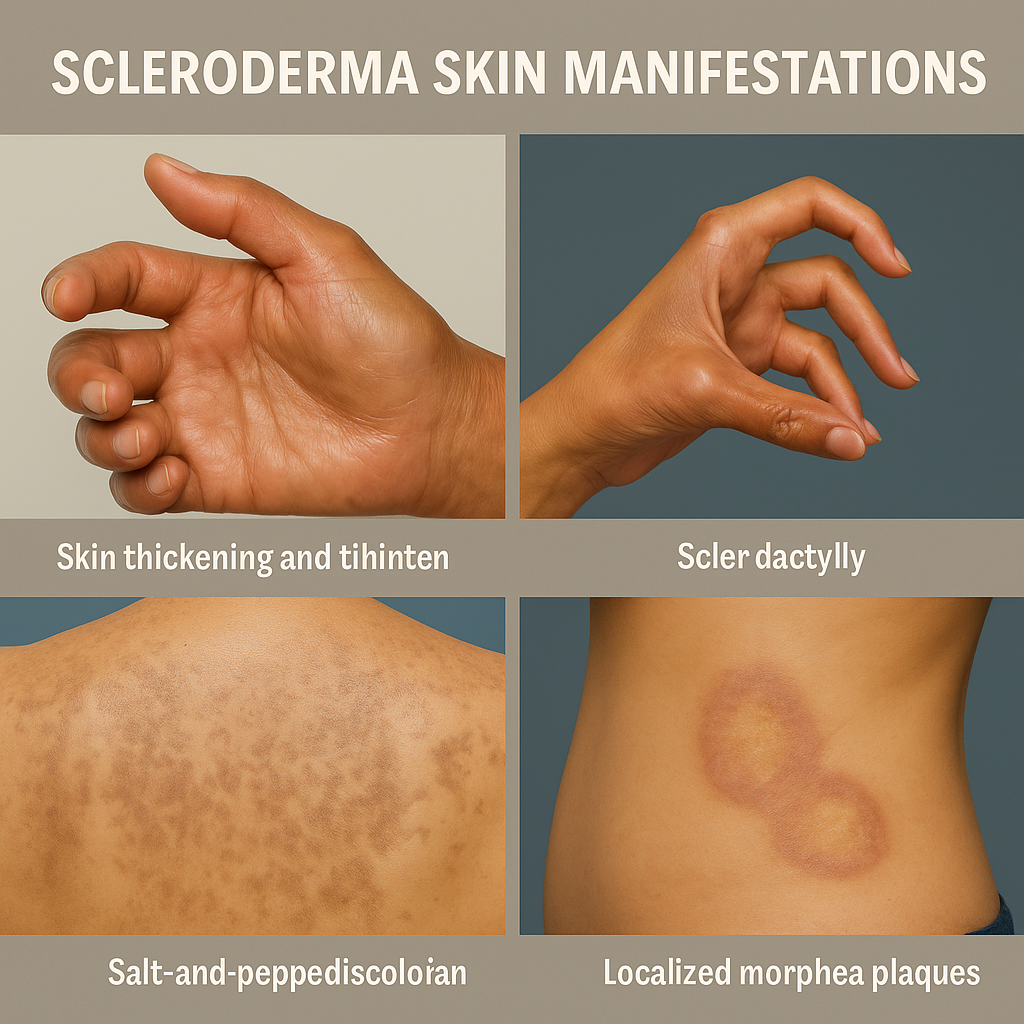
June marks National Scleroderma Awareness Month, drawing attention to a chronic autoimmune disease that affects the skin, internal organs, and vascular system. Scleroderma, meaning “hard skin,” varies dramatically in severity and presentation, complicating both diagnosis and treatment. For hospital executives and clinical leaders, this observance is an opportunity to reevaluate institutional readiness to manage complex rare diseases. Early diagnosis and coordinated care can dramatically alter outcomes, yet patients often experience delays due to misdiagnosis and fragmented specialty referrals. Systemic sclerosis, the most severe form, involves life-threatening complications such as pulmonary hypertension, renal crisis, and gastrointestinal dysfunction. Strategic hospital involvement in multidisciplinary management—rheumatology, dermatology, pulmonology, nephrology, and cardiology—is essential. Inadequate provider familiarity with scleroderma contributes to delayed referrals and worsened patient outcomes. This month, healthcare leaders are called to implement clinical pathways that support early recognition, expedite specialist access, and improve patient quality of life. Rare disease strategy is not niche—it’s a measure of system-level compassion and competence.
Diagnosing scleroderma can be especially challenging given its protean manifestations. Patients may present with Raynaud’s Phenomenon, skin thickening, digital ulcers, or nonspecific fatigue long before systemic signs appear. According to the National Institute of Arthritis and Musculoskeletal and Skin Diseases, (NIAMS), “Symptoms of Raynaud’s Phenomenon include fingers turning white, then blue, and feeling numb or painful in response to cold temperatures or stress. Usually, the same finger(s) on both hands are affected at the same time, but sometimes only one hand or a few fingers are affected” NIAMS (2023). Hospital systems should prioritize education of frontline providers on early warning signs and support access to antinuclear antibody (ANA) testing and autoantibody panels. Establishing pathways for prompt rheumatology referrals and supporting diagnostic imaging such as high-resolution CT scans and echocardiograms are critical for early disease classification. In some cases, nailfold capillaroscopy and pulmonary function testing provide necessary insight into vascular and respiratory involvement. Hospital-based rare disease programs that integrate diagnostics across specialties help reduce care fragmentation. Electronic health records (EHR) can be leveraged to flag potential early indicators for systemic sclerosis, alerting clinicians to patterns of concern. As emphasized by Ehrenstein et al. (2019) in the NCBI’s Tools and Technologies for Registry Interoperability, “EHR data can be used to support clinical care and to populate quality improvement registries by automating the identification of eligible patients based on clinical patterns and diagnostic codes.” As more is learned about the disease’s immunologic underpinnings, precision diagnostics will play an increasing role. Institutional commitment to early and accurate diagnosis transforms lives—and saves costs downstream. Scleroderma care must begin with clinical vigilance and system-wide coordination.
Effective treatment for scleroderma requires both pharmacologic innovation and integrated support services. Immunosuppressants, endothelin receptor antagonists, and antifibrotic therapies are central to management, yet medication access varies widely based on insurance coverage and geography. Hospital pharmacy teams and care navigators are of equal essential on ensuring continuity of care. Equally important, physical and occupational therapy, mental health services, wound care, and nutritional support all contribute to better functional outcomes. Leaders must champion multidisciplinary clinics and coordinated care teams that centralize services for patients who often navigate multiple providers. Telehealth expansion can also close access gaps for rural or mobility-limited patients. As Xiang and Bernard (2021) explain, “Patients identifying as non-Hispanic Black, Hispanic, or of other non-white race/ethnicity were less likely to have access to video telemedicine services, reflecting persistent digital inequities in healthcare delivery” Xiang & Bernard (2021). As outlined in the latest EULAR guidance, evidence-based recommendations from the Scleroderma Foundation and European League Against Rheumatism should inform protocol development. In the era of value-based care, scleroderma programs aligned with quality metrics, reduced hospitalizations, and improved patient satisfaction represent strategic institutional investments. Holistic, team-based models are not aspirational—they are essential for treating chronic systemic disease. Scleroderma care must be grounded in access, innovation, and empathy.
Scleroderma affects approximately 300,000 Americans, with a disproportionate burden on women and people of color. Black and Asian patients with scleroderma often present with more severe disease phenotypes and worse prognoses, a reality compounded by historical underrepresentation in clinical research. Hospital DEI strategies must include rare disease equity—ensuring culturally competent care, representative patient education materials, and diverse research participation. As Baynam et al. (2024) note, “rare disease clinical research must proactively integrate DEI principles, particularly in genetic diversity, to ensure findings are generalizable and relevant to affected populations” Baynam et al. (2024). Language access, socioeconomic barriers, and healthcare navigation challenges should be actively addressed through institutional policy. Moreover, patients with scleroderma often report being dismissed or misdiagnosed, further exacerbating mistrust and disengagement. Embedding patient-centered metrics in quality improvement efforts can surface gaps in equity and experience. Community partnerships, advocacy collaborations, and patient advisory boards can inform systemic change. True health equity means not only eliminating disparities but proactively designing care that is inclusive, representative, and affirming. Awareness months are moments to examine who is excluded and why. Hospital leaders must lead equity not just with policies—but with measurable action.
Executives and administrators hold the influence to shape systemwide responses to rare autoimmune conditions like scleroderma. From funding dedicated clinics to embedding rare disease competencies in continuing education, leadership decisions impact every level of patient care. Hospitals should evaluate their current approach to rare disease navigation and consider models that center multidisciplinary collaboration and early intervention. Notably, hospital teams can host educational events, supporting staff certifications in rheumatologic care, and sponsor rare disease research initiatives to drive institutional progress. National Scleroderma Awareness Month is not merely symbolic—it’s a call for operational change. Strategic investments in rare disease readiness improve institutional reputation, build patient trust, and enhance overall care quality. Leading on scleroderma means leading with vision, empathy, and evidence. Systemic sclerosis may be rare, but its lessons are universal: coordinated care, early action, and compassionate leadership make all the difference. As one peer-reviewed study states, “hospital leaders must seize opportunities to integrate decision-support tools and equity prompts directly into the electronic health record” Xiang & Bernard (2024). This June, let scleroderma remind us of the human imperative behind every executive decision. Leadership in rare disease is leadership in healthcare excellence.
Discover More
National Scleroderma Awareness Month offers healthcare systems a chance to reevaluate how they identify, diagnose, and support patients with rare and complex conditions. From improving care pathways to advancing equity in rheumatologic disease, hospital leaders are uniquely positioned to drive change. Begin by assessing your system’s current approach to chronic autoimmune conditions—then use this month as a launch point for strategic transformation.
Internal Resources
External Resources
- Scleroderma Foundation – Awareness Month Resources
- NIH – National Institute of Arthritis and Musculoskeletal and Skin Diseases (NIAMS)
- American College of Rheumatology – Scleroderma Fact Sheet
- Frontiers in Medicine – Racial Disparities in Systemic Sclerosis
- National Institute of Arthritis and Musculoskeletal and Skin Diseases (NIAMS). (2024). Raynaud’s phenomenon. U.S. Department of Health & Human Services, National Institutes of Health. Retrieved from https://www.niams.nih.gov/health-topics/raynauds-phenomenon
- Ehrenstein V, Kharrazi H, Lehmann H, et al. Obtaining Data From Electronic Health Records. In: Gliklich RE, Leavy MB, Dreyer NA, editors. Tools and Technologies for Registry Interoperability, Registries for Evaluating Patient Outcomes: A User’s Guide, 3rd Edition, Addendum 2 [Internet]. Rockville (MD): Agency for Healthcare Research and Quality (US); 2019 Oct. Chapter 4. Available from: https://www.ncbi.nlm.nih.gov/books/NBK551878/
- Xiang XM, Bernard J. Telehealth in Multiple Sclerosis Clinical Care and Research. Curr Neurol Neurosci Rep. 2021 Feb 28;21(4):14. doi: 10.1007/s11910-021-01103-4. PMID: 33646409; PMCID: PMC7917521.
- Del Galdo, F., Lescoat, A., Conaghan, P. G., Bertoldo, E., Čolić, J., Santiago, T., Suliman, Y. A., Matucci-Cerinic, M., Gabrielli, A., Distler, O., Hoffmann-Vold, A.-M., Castellví, I., Balbir-Gurman, A., Vonk, M., Ananyeva, L., Rednic, S., Tarasova, A., Ostojic, P., Boyadzhieva, V., El Aoufy, K., … Allanore, Y. (2025). EULAR recommendations for the treatment of systemic sclerosis: 2023 update. Annals of the Rheumatic Diseases, 84(1), 29–40. https://doi.org/10.1136/ard-2024-226430
- Baynam G, Baker S, Steward C, Summar M, Halley M, Pariser A. Increasing Diversity, Equity, Inclusion, and Accessibility in Rare Disease Clinical Trials. Pharmaceut Med. 2024 Jul;38(4):261-276. doi: 10.1007/s40290-024-00529-8. Epub 2024 Jul 9. PMID: 38977611.
- Stoesz A, Joers B, Gaviglio A. Hospital administrators as forgotten partners in rare disease care: a call to action by the international hospital federation’s global rare pediatric disease network. Orphanet J Rare Dis. 2024 Dec 4;19(1):456. doi: 10.1186/s13023-024-03459-5. PMID: 39633381; PMCID: PMC11616372.

{kind=link}
{kind=link}
{kind=link}